Shell shock.
Battle Fatigue.
Combat Stress Reaction.
Over the past 110 years, a number of colloquial terms and medical diagnoses have been used to describe what we now call “Post-Traumatic Stress,” but they each describe the invisible wounds of war which manifest through nightmares, flashbacks, depression, anger, shame, anxiety, panic, tremors, insomnia, headaches, guilt, memory loss, gastrointestinal issues and more.
SHELL SHOCK AND THE FIRST WORLD WAR
In 1915, as the Great War was raging across Europe, soldiers were suffering. Wounds and fatalities were high and even those who emerged from the trenches without physical injuries were hiding emotional scars; that’s when medical officer Charles Myers coined the term “Shell Shock” to describe what was believed to be “a physical injury to the nervous system during a heavy bombardment.” The first identified patient to be suffering from post-traumatic stress had survived an explosive attack in France that left him temporarily unable to speak. He was hospitalized for three months, during which time his weak limbs seemed to strengthen and he regained speech, but he developed a tremor so intense he could not shave, struggled to eat and lost the ability to stand.1 In the aftermath of the war, more than a quarter of a million allied veterans were suffering from this “mysterious” and misunderstood ailment, but treatment for many was inaccessible or nonexistent, and those who did receive treatment were rarely truly helped by it, as the methods employed at the time included electroshock therapy, underdeveloped psychotherapy techniques and commitment to psychiatric asylums.2
THEY DIDN’T TALK ABOUT IT
World War II saw trench warfare steadily being replaced by armored warfare, as more of the fighting was happening using tanks and planes than in the previous war, though close combat continued.
During World War II, the number of fatalities both of Americans and worldwide more than tripled those of World War I, and while the ceasefires of V-E Day and V-J Day meant soldiers could finally return home to their families, thousands came home with the invisible battle scars of “combat fatigue.” It was believed by many that the trauma of war was not necessarily caused by the horrors faced, but by the length of time one spent facing them without rest. According to the National World War II Museum, “It was determined by the U.S. Army that the breaking point for a soldier on the front line was somewhere between 60 and 240 days, depending on the intensity and frequency of combat.”3
While medical professionals and psychologists were on their way to better understanding the condition, they erroneously believed that those who suffered from this trauma must have had “pre-existing mental conditions,” thus their belief was that prevention meant determining before deployment which soldiers might be susceptible and dismissing them from duty. They were steadfastly proven wrong, though, as the number of soldiers suffering from signs of psychological trauma rivaled that of the previous war and continued to rise.
Specifically regarding those who served during Operation Overlord (the battle of Normandy; 81 years ago this month), the effectiveness of individual troops dropped considerably after one month of fighting; by day 45, some were in a near-vegetative state.3
Clearly combat, and, in particular, continued combat requiring constant vigilance, seemed to greatly increase the likelihood of developing post-traumatic stress, regardless of the individual’s previous experiences or general well-being prior to battle. In other words, PTS was not caused by a pre-existing condition. By the war’s end, nearly 40% of those who had obtained a medical discharge were suffering primarily, if not entirely, from “combat fatigue” and psychological stress. This continued with Korea and Vietnam, with “Post-Vietnam Syndrome” even the go-to term for post-traumatic stress for a period.
Unfortunately, many veterans of these conflicts decided upon returning home that they would never discuss the truly horrific experiences on the battlefields, choosing instead to bury their pain, attempt to drink it away and/or suffer silently.
“There was a generation of folks who had tremendous trauma and pain and that overflowed into their families in ways that we still can’t even quantify,” Founder and CEO of Iraq and Afghanistan Veterans of America Paul Rieckhoff told CNN in 2023. Reickhoff’s veteran grandfather had been a prisoner of war at Stalag Luft III during World War II. Survivors weren’t talking about their trauma, which meant they weren’t receiving treatment for their trauma.
Wilbert “Tex” Dettman was one of those veterans. We interviewed his daughter, Cheryl Hurley, of Auxiliary 5446 in Plainfield Connecticut, ahead of Pearl Harbor Day in 2022. Her father was awaiting his next orders on base when the December 7, 1941 attack started. “He ended up pulling bodies out of the water… for two days without any sleep,” said Hurley. “They ended up burning their uniforms because (of the) ash and blood. (They) were totally destroyed.”
Dettmann, a Purple Heart recipient who was erroneously listed missing in action in the aftermath, was one of countless soldiers to suffer from Post-Traumatic Stress (PTSD) as a result.
Said Hurley, “A loud noise would send him to the floor.”
Dettman rarely spoke of his experiences. He passed away in 2011.
Over the last several decades, developments in the field of psychology and an emphasis on talk therapy led to a better understanding of “combat fatigue” and “shell shock,” and in 1980, Post-Traumatic Stress Disorder was classified as an anxiety disorder by the American Psychiatric Association.4 Requirements for the diagnosis included exposure to a stressful event; in recent years, a growing movement has pushed for the term to be changed from Post Traumatic Stress Disorder to post-traumatic stress, which falls under Trauma and Stressor-Related Disorders in the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition). The intention is to classify PTS as an injury and a symptom rather than its own disorder; this is believed to be a step in the direction of de-stigmatizing it and thereby encouraging veterans to seek help.
According to a U.S. Department of Veterans Affairs report in 2018, fewer than half of veterans with this diagnosis seek treatment; at that time, 20 veterans were dying by suicide each day.4
Today, there are a number of effective treatments for post-traumatic stress and related disorders, including antidepressant and anxiety medications, cognitive therapy and exposure therapy (under the guidance of qualified professionals). According to the website of the VA, treatment is available for any veteran suffering from the effects of post-traumatic stress, including both outpatient and residential care dependent upon one’s needs.5
Unfortunately, barriers continue to exist, and one of these is the social stigma surrounding mental health. VFW National Headquarters and leadership therefore feel it is important to remind veterans that asking for help “is a sign of strength, not weakness.” Their recent statement goes on to say, “Navigating the complexities of PTSD and other mental health conditions can be a challenging and isolating journey, which is why connecting with brothers and sisters-in-arms who share similar experiences can be incredibly powerful. Within the VFW’s nearly 6,000 Posts worldwide, veterans find safe spaces where they can share experiences without judgement, speak freely and receive authentic camaraderie.”
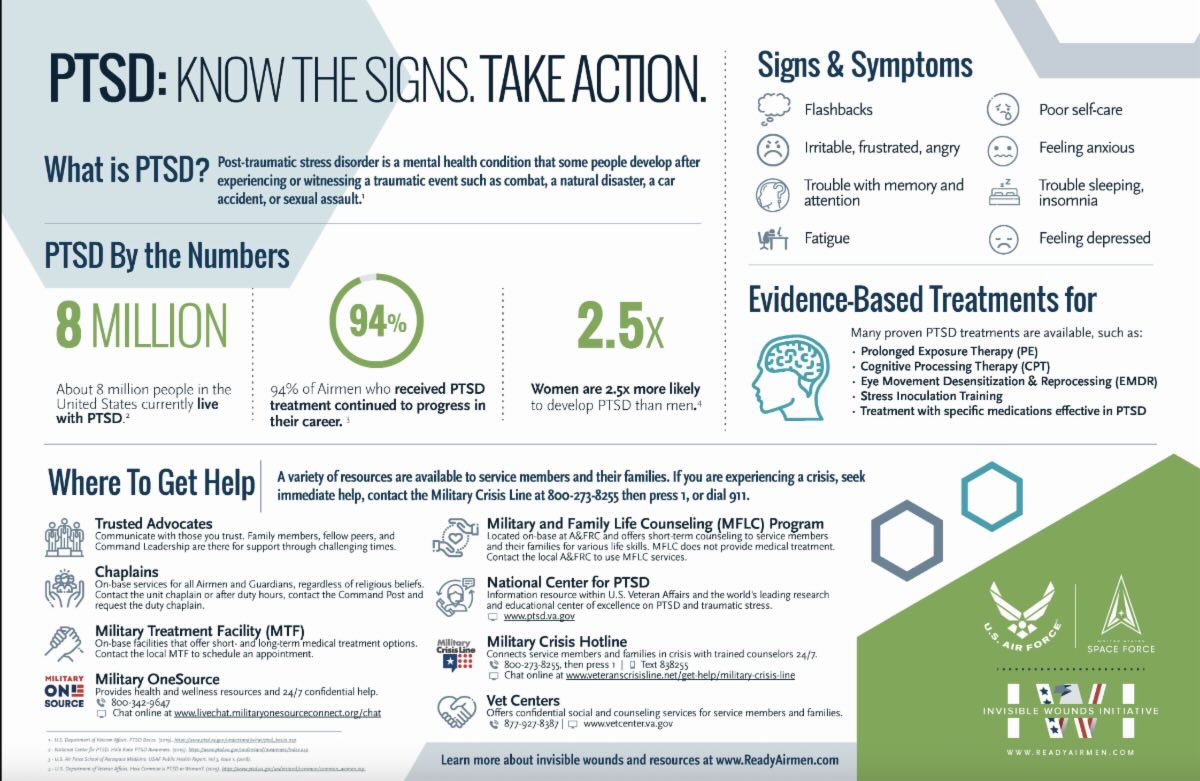
The first step toward helping people with post-traumatic stress is being able to identify post-traumatic stress. Print out the below graph as a handy guide you can keep with you, courtesy of the U.S. Air Force site.